
MEDICO-LEGAL ANNUAL REPORT 2025

ROMIC CARE FOUNDATION
@ ROMIC MEDICAL CENTRE – JINJA
“Dignity & Quality Life for All”
2025 MEDICO-LEGAL ANNUAL REPORT
January – December 2025
Jinja, Uganda
2026
Table of Contents
1.1. Organizational Overview 1
1.3. Vision, Mission, Strategic Goal, and Slogan 2
1.4. Legal Status and Registration 3
4.0 OVERALL CASELOAD SUMMARY 6
4.2 Case Distribution (Survivors) 6
6.0 GENDER-BASED VIOLENCE (GBV) ANALYSIS 11
7.0 GEOGRAPHIC DISTRIBUTION 13
8.1 Sex Distribution (Survivors) 16
9.0 CLINICAL & FORENSIC FINDINGS 17
9.2 Pregnancy (HCG) Testing 19
9.3 Duration to Examination 19
11.3 Prevention & Community Engagement 22
ACKNOWLEDGEMENT
Romic Care Foundation extends sincere appreciation to:
- Survivors and clients who entrusted us with their care.
- The medical team whose dedication ensured quality medico-legal documentation.
- The Uganda Police Force and judicial officers for continued collaboration.
- Local leaders (LCI/LCII) who facilitate referrals at community level.
- Development partners and well-wishers supporting our mission.
We especially recognize our frontline Doctors/clinicians who continue to work under resource limitations to ensure that justice and health services remain accessible to vulnerable populations.
ABBREVIATIONS
| Abbreviation | Meaning |
|---|---|
| GBV | Gender-Based Violence |
| DV | Domestic Violence |
| HIV | Human Immunodeficiency Virus |
| HCG | Human Chorionic Gonadotropin (Pregnancy Test) |
| PEP | Post-Exposure Prophylaxis |
| STI | Sexually Transmitted Infection |
| RTA | Road Traffic Accident |
| LCI/LCII | Local Council I / II |
| SOCO | Scene of Crime Officer |
| ROCAF | Romic Care Foundation |
EXECUTIVE SUMMARY
In 2025, Romic Care Foundation documented 4,740 medico-legal clients, including:
- 4,346 survivors/victims
- 421 suspects/perpetrators
The organization continues to operate at the intersection of health and justice, providing medical examinations, forensic documentation, court testimony, and counselling services.
Key Highlights
- Common assault accounted for 2,630 survivors (60.5%).
- GBV burden remains high, including:
- Defilement (simple + aggravated): 428 cases
- Domestic violence: 663 cases
- Other GBV: 189 cases
- Rape: 40 cases
- Geographic concentration:
- Jinja City – 58.31%
- Buikwe – 24.58%
- Jinja District – 13.40%
- 100 court appearances were made by medical professionals.
- HIV positivity among those tested remained below 3%.
- Pregnancy positivity among tested female survivors was 23.35%.
- Most sexual assault survivors presented after 3–7 days, limiting preventive intervention.
Despite limited resources, the Foundation provided:
- First-contact counselling to all clients
- Basic medical management
- Forensic documentation for justice processes
However, transport barriers, delayed reporting, limited forensic capacity, and resource constraints remain critical gaps.
1.0 ORGANIZATIONAL PROFILE
1.1. Organizational Overview
Romic Care Foundation (ROCAF) is an indigenous Community-Based Organization (CBO) operating in Uganda. The organization works primarily in peri-urban and hard-to-reach rural communities, supporting vulnerable and marginalized populations—especially survivors of Gender-Based Violence (GBV), children, and youth.
ROCAF operates through Romic Medical Centre Jinja, providing integrated health, medico-legal, and social support services.
1.2. Background and Origin
Romic Care Foundation was founded in 2017 following a life-changing experience during one of its founder’s internships at Jinja Regional Referral Hospital in 2014.
While working in the Medico-Legal Department, he witnessed firsthand the devastating consequences of Gender-Based Violence (GBV) and the severe gaps in survivor-centered services.
One case that profoundly shaped the organization’s birth involved a 15-year-old girl who had been raped and was forced to seek help three times before receiving medical attention. Due to delays in accessing Post-Exposure Prophylaxis (PEP) and Emergency Contraceptive Prophylaxis (ECP), she later tested positive for HIV.
That experience and many similar cases revealed systemic failures in timely response, survivor protection, and coordinated care. In response, ROCAF was established with the primary goal of improving access to timely, professional medical services for survivors of GBV.
Initially operating as a medical center, ROCAF soon recognized that survivors required far more than medical care alone. The organization therefore evolved into a foundation, expanding its scope to address broader social, economic, and justice-related needs of vulnerable communities.
A Tragedy That Could Have Been Prevented
In December 2023, ROCAF encountered a deeply painful case that exposed critical weaknesses in Uganda’s emergency response systems.
A 16-year-old girl from Bugembe, under pressure from her boyfriend, underwent an unsafe abortion. When complications arose, her frightened parents took her to the police station instead of directly to a health facility, believing this was the appropriate first step.
Time was lost at the police station. Statements were recorded, but due to lack of emergency coordination and transport facilitation, she remained without urgent medical care for several hours.
By the time she arrived at ROCAF’s medical center, her condition had severely deteriorated. Our team provided immediate first aid and clinical assessment. However, her condition required advanced emergency intervention beyond our facility’s capacity. She was urgently referred to Jinja Regional Referral Hospital.
Tragically, due to fear, confusion, and possible financial constraints, she was taken back home instead. Days later, we learned that she had eventually reached the referral hospital but it was too late. She had passed away.
Her death was not merely a medical failure. It was a systems failure.
It was the result of:
- Delayed care
- Lack of coordinated emergency referral
- Stigma
- Limited survivor-centered services
- Absence of a fully equipped One-Stop Crisis Centre
A fully functional crisis center could have saved her life. It could still save the next girl.
1.3. Vision, Mission, Strategic Goal, and Slogan
Vision:
Dignity and quality life for all.
Mission:
To empower marginalized and vulnerable communities through integrated solutions in health, education, gender equality, WASH, climate resilience, and socio-economic empowerment to promote social justice, human rights, and sustainable development.
Strategic Goal:
To create lasting positive change through comprehensive programs that promote resilience, equity, inclusivity, and sustainable livelihoods.
Slogan:
Building a brighter future together.
1.4. Legal Status and Registration
Romic Care Foundation is:
- Registered with Jinja District Local Government (since 2018)
- Registered with Jinja City (2023)
- Incorporated as a Company Limited by Guarantee (non-shareholding entity)
1.5. Core Values
- Compassion and empathy
- Inclusivity and equity
- Resilience and sustainability
- Accountability and integrity
1.6. Theory of Change
ROCAF’s approach addresses the root causes of poverty, Gender-Based Violence, and social injustice by empowering communities with skills, knowledge, and access to services. By strengthening systems and building resilience, communities can break cycles of vulnerability and achieve sustainable livelihoods.
2.0 INTRODUCTION
This report provides a comprehensive analysis of medico-legal services delivered by Romic Care Foundation between January and December 2025.
The objectives are to:
- Describe annual caseload trends
- Examine GBV patterns
- Analyze geographic distribution
- Identify system and service gaps
- Inform prevention and policy planning
All findings are derived strictly from the 2025 medico-legal register and a cleaned geographic dataset (village–district mapping) prepared from the same.
Romic Care Foundation operates at the intersection of health and justice, supporting survivors, examining suspects, and providing expert evidence to courts. The numbers in this report represent real people, families and communities facing violence and trauma and the efforts of a small but committed team to respond.
3.0 METHODOLOGY
- All entries in the register were treated as 2025 cases.
- Addresses were corrected and standardized.
- District totals were validated to ensure no duplication.
- GBV categories included:
- Aggravated defilement
- Defilement
- Domestic violence
- Child abuse
- Rape
- Other GBV
- Totals were verified to align with the grand total of 4,740.
Limitations include incomplete documentation for HIV, pregnancy testing, and duration in some cases.
4.0 OVERALL CASELOAD SUMMARY
4.1 Total Clients: 4,740
- Survivors/Victims: 4,346
- Suspects/Perpetrators: 421
4.2 Case Distribution (Survivors)
| CASE TYPE | # OF SURVIVORS/VICTIMS | ||
| F | M | TOTAL | |
| AGG DEFILEMENT | 52 | 10 | 62 |
| DEFILEMENT | 359 | 7 | 366 |
| COMMON ASSAULT | 733 | 1897 | 2630 |
| CHILD ABUSE | 24 | 36 | 60 |
| DOMESTIC VIOLENCE | 490 | 173 | 663 |
| OTHER GBV | 149 | 40 | 189 |
| RAPE | 40 | 0 | 40 |
| ANCEST | 1 | 0 | 1 |
| ABORTION | 4 | 0 | 4 |
| DOGBITE | 16 | 16 | 32 |
| ROAD TRAFFIC ACCIDENT | 75 | 224 | 299 |
| TOTAL | 1943 | 2403 | 4346 |
Table 1: Category of all cases (survivors) recorded in 2025
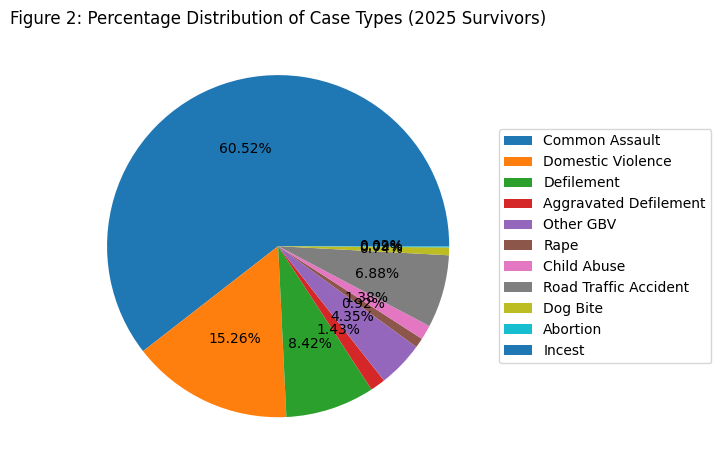
Figure 1 Pie Chart – Percentage Distribution of Case Types
Common assault dominates, followed by domestic violence and defilement.
Sexual violence disproportionately affects females, while common assault affects more males.
4.3 SUSPECTS & PERPETRATORS
| CATEGORY | Female (F) | Male (M) | TOTAL | % of All Suspects |
|---|---|---|---|---|
| Suspects in sexual assault | 4 | 179 | 183 | 43.47% |
| Suspects in non-sexual assault | 27 | 211 | 238 | 56.53% |
| TOTAL | 31 | 390 | 421 | 100% |
Table 2. Category of Suspect/Perpetrator (n = 421)
The overwhelming majority of suspects are male, particularly in sexual assault. ROMIC’s medico-legal services thus support justice for survivors while preserving due process for suspects.
The team was summoned as professional witnesses in 100 cases, providing expert evidence in both magistrate and high courts.
5.0 TIME TRENDS ANALYSIS
5.1 Weekly Distribution
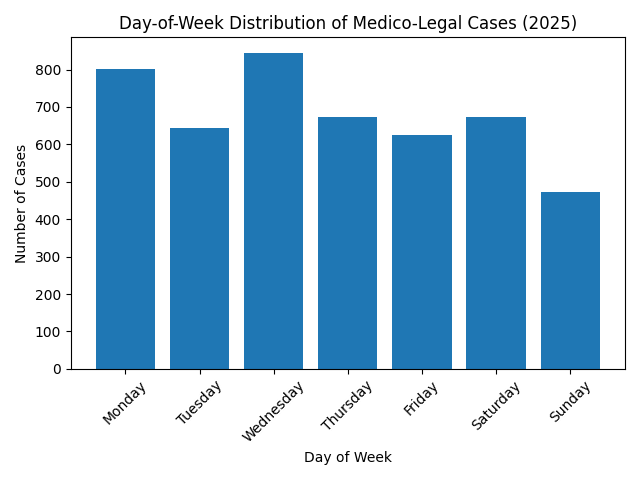
Figure 2Bar Chart shows Distribution of cases through the week
Narrative – Weekly Patterns
- Wednesday (17.8%) recorded the highest number of cases.
- Monday (16.9%) is also significantly high.
- Sunday (10%) recorded the lowest.
Interpretation:
- The high numbers on Monday and Wednesday may indicate:
- Incidents occurring over the weekend and reported early in the week.
- Police and institutional processes being more active mid-week.
- Lower Sunday numbers likely reflect:
- Reduced facility attendance
- Transportation challenges
- Survivors waiting until weekday services resume
- The pattern suggests that violence frequently occurs during weekends, but reporting often happens during weekdays when formal systems are accessible.
Overall Time Trend Interpretation
- Violence is consistent throughout the year, not limited to isolated periods.
- Peaks in late Q3 (August–September) suggest potential need for:
- Targeted seasonal prevention campaigns
- Increased staffing during high-burden months
- Weekly trends indicate the importance of:
- Ensuring service readiness on Mondays
- Strengthening weekend reporting mechanisms.
5.2 Monthly Distribution
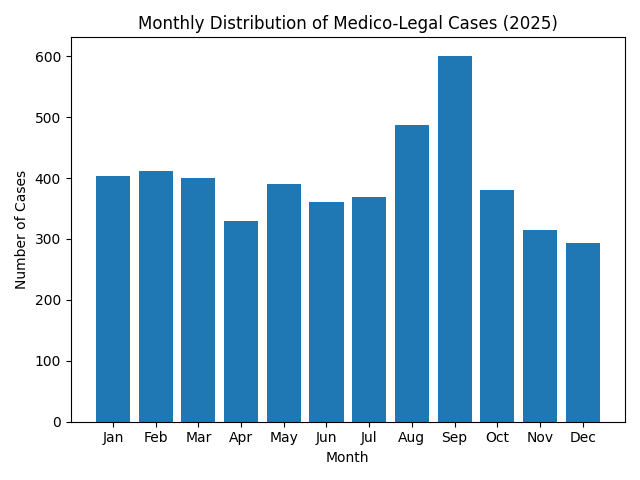 Figure 3Bar Chart shows the Distribution of cases through the month
Figure 3Bar Chart shows the Distribution of cases through the month
Narrative – Monthly Trends
- September recorded the highest caseload (12.68%), making it the peak month.
- August (10.27%) was the second highest.
- The lowest months were:
- December (6.18%)
- November (6.62%)
- April (6.96%)
Interpretation:
- There is a noticeable surge in cases during August and September, possibly linked to:
- School holidays and increased child exposure to risk
- Seasonal economic stressors
- Increased community mobility
- Lower reporting in November and December may reflect:
- Holiday travel
- Reduced institutional operations
- Community focus on festivities rather than reporting violence
- The distribution across the year is relatively steady, indicating that violence is not seasonal alone but persistent throughout the year, with periodic spikes.
6.0 GENDER-BASED VIOLENCE (GBV) ANALYSIS
6.1 GBV Burden.
For this report, GBV includes:
• Domestic violence
• Simple defilement
• Aggravated defilement
• Child abuse
• Other GBV
• Rape
• Incest (ANCEST)
From Table 1:
• Defilement (simple + aggravated): 428 survivors
• Domestic violence: 663 survivors
• Other GBV: 189 survivors
• Rape: 40 survivors
• Child abuse: 60 survivors
• Incest: 1 survivor
Together, these categories represent well over a quarter of all survivors and are heavily concentrated among women and children.
6.2 GBV by Major District.
From the cleaned district-level data:
• Jinja City: 2,764 total medico-legal cases (58.31%)
• Buikwe: 1,165 cases (24.58%)
• Jinja District: 635 cases (13.40%)
These three account for 96.29% of all recorded cases. GBV mirrors this pattern, with the majority of GBV cases originating from Jinja City and Buikwe.
6.3 Interpretation
• Jinja City is the primary GBV hotspot, reflecting urban density, higher reporting, and proximity to the facility.
• Buikwe is a major secondary hotspot, reflecting strong population movement and referral linkages to Jinja.
• Jinja District has lower recorded numbers, but this is likely due to access constraints, not lower violence:
o Transport difficulties from rural areas
o Cases handled at nearby facilities that may lack full medico-legal capacity
o Delays at the village and police level before referral
For funders: This is a critical area where support for transport, outreach, and decentralized medico-legal capacity could dramatically increase timely GBV response.
7.0 GEOGRAPHIC DISTRIBUTION
7.1 Village Contribution
| DISTRICT | VILLAGE | NUMBER_OF_CASES |
| AMOLATA | AMOLATA | 1 |
| BUGIRI | BUGIRI | 4 |
| BUGWERI | BUGWERI | 3 |
| BUIKWE | WAKISI | 381 |
| BUIKWE | MBIKO | 267 |
| BUIKWE | NJERU | 238 |
| BUIKWE | LUGAZI II | 117 |
| BUIKWE | NYENGA | 97 |
| BUIKWE | BUKAYA | 65 |
| BUIKWE | BUIKWE | 28 |
| BUIKWE | KONKO | 23 |
| BUIKWE | LUGAZI | 15 |
| BUIKWE | KUNKU KAWULE | 1 |
| BUSEMBATYA | BUSEMBATYA | 1 |
| BUVUMA | BUVUMA | 6 |
| IGANGA | IGANGA | 17 |
| JINJA CITY | MAFUBIRA | 701 |
| JINJA CITY | MASESE | 520 |
| JINJA CITY | BUGEMBE | 498 |
| JINJA CITY | WANYANGE | 234 |
| JINJA CITY | BUDONDO | 240 |
| JINJA CITY | JINJA TOWN | 237 |
| JINJA CITY | MPUMMUDDE | 234 |
| JINJA CITY | LWANDA | 29 |
| JINJA CITY | KISIMA | 4 |
| JINJA DISTRICT | KAKIRA | 368 |
| JINJA DISTRICT | BUWENGE | 101 |
| JINJA DISTRICT | BUYENGO | 56 |
| JINJA DISTRICT | NAMAGANGA | 31 |
| JINJA DISTRICT | BUTAGAYA | 27 |
| JINJA DISTRICT | WAIRAKA | 52 |
| KAMPALA | KAMPALA | 22 |
| KAMULI | KAMULI | 12 |
| KAYUNGA | KAYUNGA | 12 |
| KENYA | KENYA | 9 |
| KISORO | KISORO | 1 |
| KUMI | KUMI | 1 |
| LUUKA | LUUKA | 16 |
| MAYUGE | MAYUGE | 33 |
| MBALE | MBALE | 4 |
| MITIYANA | MITIYANA | 2 |
| MOROTO | MOROTO | 1 |
| MUBENDE | MUBENDE | 1 |
| MUKONO | MUKONO | 10 |
| NAMUTUMBA | NAMUTUMBA | 4 |
| PALISA | PALISA | 2 |
| RWANDA | RWANDA | 2 |
| TORORO | TORORO | 2 |
| WAKISO | WAKISO | 10 |
| TOTAL | 4740 |
Table 3. Village level Case Distribution (n=4740)
7.2 District Contribution
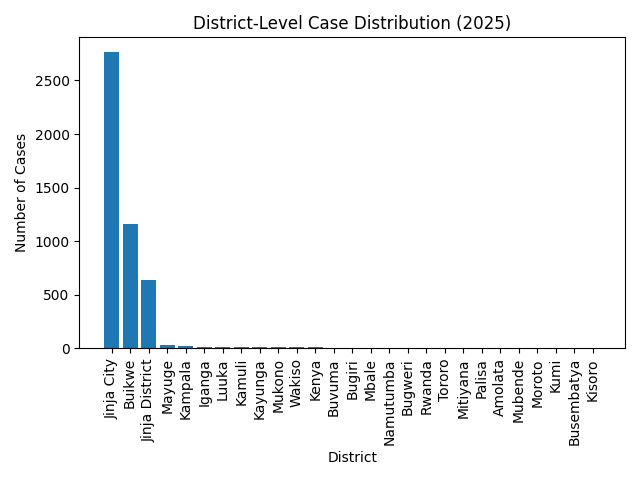
Figure 4Bar chart shows Distribution of case at District level
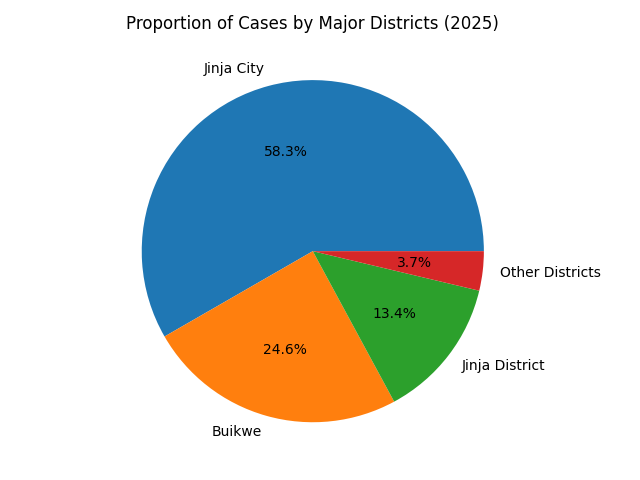
Figure 5Pie-Chart shows Percentage Distribution of cases by Major Districts
8.0 DEMOGRAPHIC OVERVIEW
8.1 Sex Distribution (Survivors)
From Table 1:
- Female survivors: 1,943
- Male survivors: 2,403
Sex distribution varies heavily by case type:
- Sexual violence & DV: Mostly female.
- Common assault & RTA: Higher proportion of males.
8.2 Age Distribution
| Age band (years) | Number | % of cases with age recorded |
|---|---|---|
| 0–9 | 128 | 2.7% |
| 10–17 | 640 | 13.6% |
| 18–24 | 1,119 | 23.8% |
| 25–34 | 1,474 | 31.4% |
| 35–49 | 1,005 | 21.4% |
| 50–64 | 284 | 6.0% |
| 65–90 | 47 | 1.0% |
Table 4. Age Distribution of All Cases (n ≈ 4,697 recorded ages)
Most survivors are young adults (18–34 years), but there is also a significant burden among children and adolescents, especially in defilement and child abuse cases.
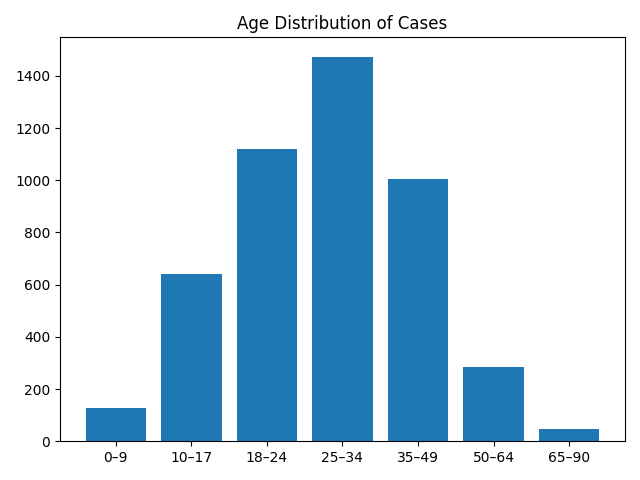
Figure 6 Bar Chart – Age Distribution of Survivors
9.0 CLINICAL & FORENSIC FINDINGS
9.1 HIV Testing
HIV test results:
- Females tested: 489
- Negative: 485
- Positive: 4 → 0.82%
- Males tested: 174
- Negative: 169
- Positive: 5 → 2.87%
Almost all tested clients were sexual assault victims. Only a few non-sexual physical assault cases were tested due to specific HIV risk (e.g. human bites).
Interpretation:
- Overall HIV positivity among those tested is low, but:
- Delayed reporting reduces the usefulness of HIV PEP and early diagnosis.
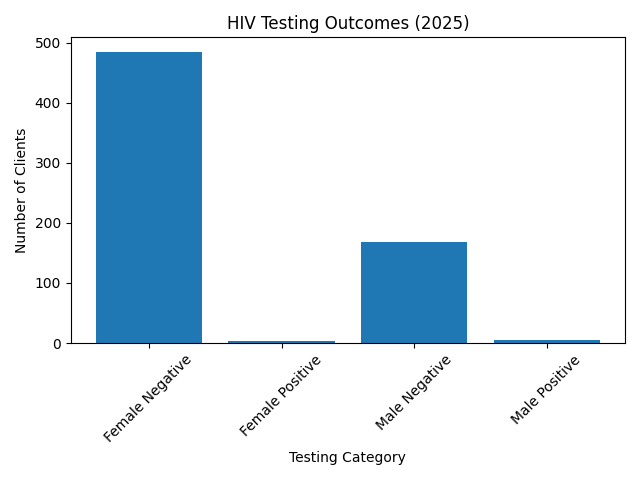
Figure 7Bar Chart outcome of HIV testing on female & males
9.2 Pregnancy (HCG) Testing
- Total females tested for pregnancy: 424
- Negative: 325
- Positive: 99 (23.35%)
Almost all pregnancy tests were done in sexual assault survivors. A very small number of non-sexual assault victims were tested due to suspected pregnancy or to rule out harm to an existing pregnancy.
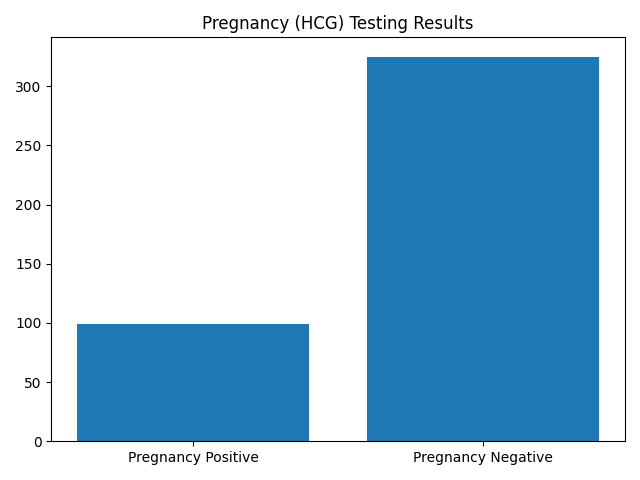
Figure 8Bar Chart shows Pregnancy Testing results
9.3 Duration to Examination
- Duration from incident to examination was standardized into days.
- Median time to presentation: approximately 3 days.
- Most sexual assault survivors presented between 3 and 7 days after the incident, beyond the ideal 72-hour window for:
- HIV post-exposure prophylaxis
- Emergency contraception
- Reasons for delay include:
- Trying to resolve cases at village/LCI level first
- Time lost at police during statement-taking
- Lack of transport and facilitation to reach the medico-legal centre
- Fear, stigma, and self-blame (especially for rape survivors)
- Minors afraid to disclose due to threats or harsh caregivers
Impact of delayed reporting:
- Reduced chances to prevent HIV and other STIs
- Reduced opportunity to prevent unwanted pregnancy
- Biological evidence often lost (bathing, time lapse, contamination)
- Weaker cases in court, affecting convictions and justice outcomes
For non-sexual physical assault, especially domestic violence:
- Many survivors only report after multiple episodes.
- By the time they present, assault has already happened several times.
9.4 Biological Evidence
- Biological evidence (semen, swabs, clothing, etc.) is very poorly documented.
- Reasons:
- Most survivors arrive after 3 days, when much evidence is lost.
- Many survivors bathe, wash clothing, or clean themselves before examination because they are not taught to preserve evidence.
- Samples collected are sometimes mishandled in transit, stored incorrectly at police, and delayed before delivery to the forensic lab in Kampala.
This significantly weakens the forensic value of examinations.
For funders, this is a critical opportunity:
- Support for forensic kits,
- Training for proper sample collection & chain-of-custody,
- Transport solutions for timely referral and sample delivery.
10.0 KEY CHALLENGES
- Delayed presentation for sexual assault and domestic violence survivors.
- Transport and referral barriers, especially from rural Jinja District and surrounding areas.
- Limited forensic capacity – inadequate kits, training, and sample handling.
- Incomplete documentation for HIV, pregnancy testing, and duration to examination.
- Stigma and fear, particularly among rape survivors and minors.
- Limited resources for psychosocial care – the team offers first-contact counselling but cannot provide long-term support because of funding and staffing constraints.
- High workload concentrated in a small team, which affects ability to scale outreach and prevention.
11.0 KEY RECOMMENDATIONS
11.1 Geographic Focus
- Prioritize Jinja City, Buikwe, and Jinja District as core service areas.
- Invest in transport support (e.g., survivor referral vouchers, police–health transport linkages).
- Strengthen linkages with outlying districts (Mayuge, Luuka, Iganga, etc.) via:
- Training of local clinic staff on initial handling.
- Clear referral pathways to ROMIC facilities.
11.2 Clinical Improvement
- Standardize HIV and pregnancy testing for all eligible sexual assault cases.
- Develop a timed pathway for:
- Triage
- Forensic examination
- Documentation
- Psychosocial support
- Invest in:
- PEP drugs and emergency contraception
- Forensic evidence kits and secure storage
- Training for clinicians and police officers in medico-legal best practices.
11.3 Prevention & Community Engagement
- Community sensitization campaigns on:
- The importance of reporting within 72 hours after sexual assault.
- Encouraging survivors to preserve evidence (not to bathe/clean until after examination when possible).
- Reducing stigma around reporting, especially for women and minors.
- Partner with:
- Local leaders (LCI/LCII)
- Police
- Religious and cultural institutions
- Schools and youth groups
- Develop support groups for GBV survivors and link them to:
- Legal aid
- Psychosocial support
- Economic empowerment programs (with partners).
NB: For funders, supporting these areas could translate directly into prevented HIV infections, fewer unwanted pregnancies, stronger court cases, and safer communities.
NB: This report is therefore both an account of what has been done in 2025, and an invitation to walk alongside Romic Care Foundation to protect survivors, strengthen justice, and build safer communities.
APPROVAL AND AUTHORIZATION
This Annual Report for the period January–December 2025 has been reviewed and approved by the leadership of Romic Care Foundation. The information presented reflects data extracted from the official medico-legal register and verified institutional records.
Kanabiro Robert
______________________________
Executive Director
Romic Care Foundation
Date: ________________________
Nangendo Sophie
______________________________
Board Chairperson
Romic Care Foundation
Date: ________________________